

An invention to prevent strokes, first sketched out in hospital basements and hotel restaurants in the Twin Cities a decade ago, hit a milestone of 100,000 human implants last month in a product niche racing toward $1 billion in yearly sales.
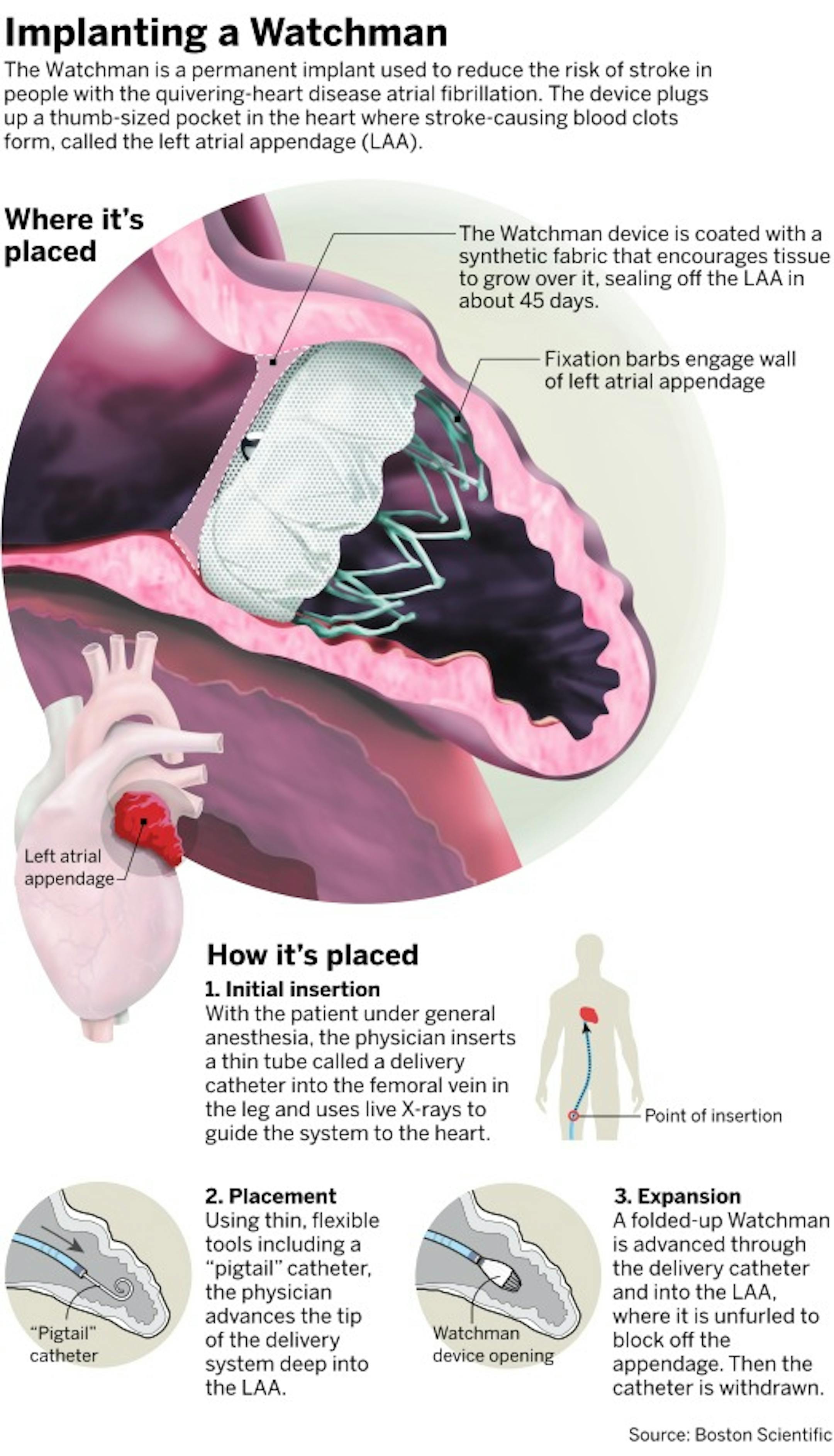
The Watchman left-atrial appendage closure device, invented at Plymouth startup Atritech and partly manufactured by 150 people at Boston Scientific in Maple Grove today, is designed to prevent strokes in people with atrial fibrillation. The pluglike system permanently seals off an obscure corridor of the heart where blood clots form when the heart is quivering, allowing patients to stop taking blood-thinning drugs.
Boston Scientific executives said the device is available at 600 U.S. hospitals, but they don't disclose pricing or revenue totals. Analysts with Decision Resources Group said U.S. hospitals pay an average $15,800 for the device, not including rebates, and Boston Scientific is on track to generate more than $500 million in U.S. sales this year.
The idea of blocking clots before they can migrate to the brain may sound straightforward today, but back in the early 2000s, it was anything but, the Watchman's inventors said.
The safety of "obliterating" the source of stroke-causing clots had to be proved, and a design using materials and techniques borrowed from stents was sketched out. Regulators applied unprecedented scrutiny. Hundreds of doctors were taught to safely prescribe and implant, and insurers were persuaded the implant could be as cheap and safe as blood thinners. Ads began flickering across TVs.
Back in late October 2003, Mayo Clinic cardiologist Dr. David Holmes, a co-inventor and co-founder of Atritech, wiped a little sweat from his brow after implanting the first Watchman in the U.S., at the Rochester hospital. "The striking thing is that now, in 2019, ... my colleague Dr. [Mohamad] Alkhouli at Mayo put in the 100,000th device that's ever been used," Holmes said in an interview.
Getting a Watchman does carry upfront health risks and costs — most complications are procedure-related, and hospitals were getting about $16,100 from Medicare to implant the nitinol-wire device under 2016 Medicare rates published last year in a study in Stroke.
But the health risks and systemic costs of taking anti-coagulation drugs mount steadily over time, unlike the Watchman, where costs and risks stabilize after a few months. The study in Stroke found that a Watchman implant becomes more cost-effective than drugs five or six years after implant, making it "more effective and less costly" in the long run.


